The fractured question
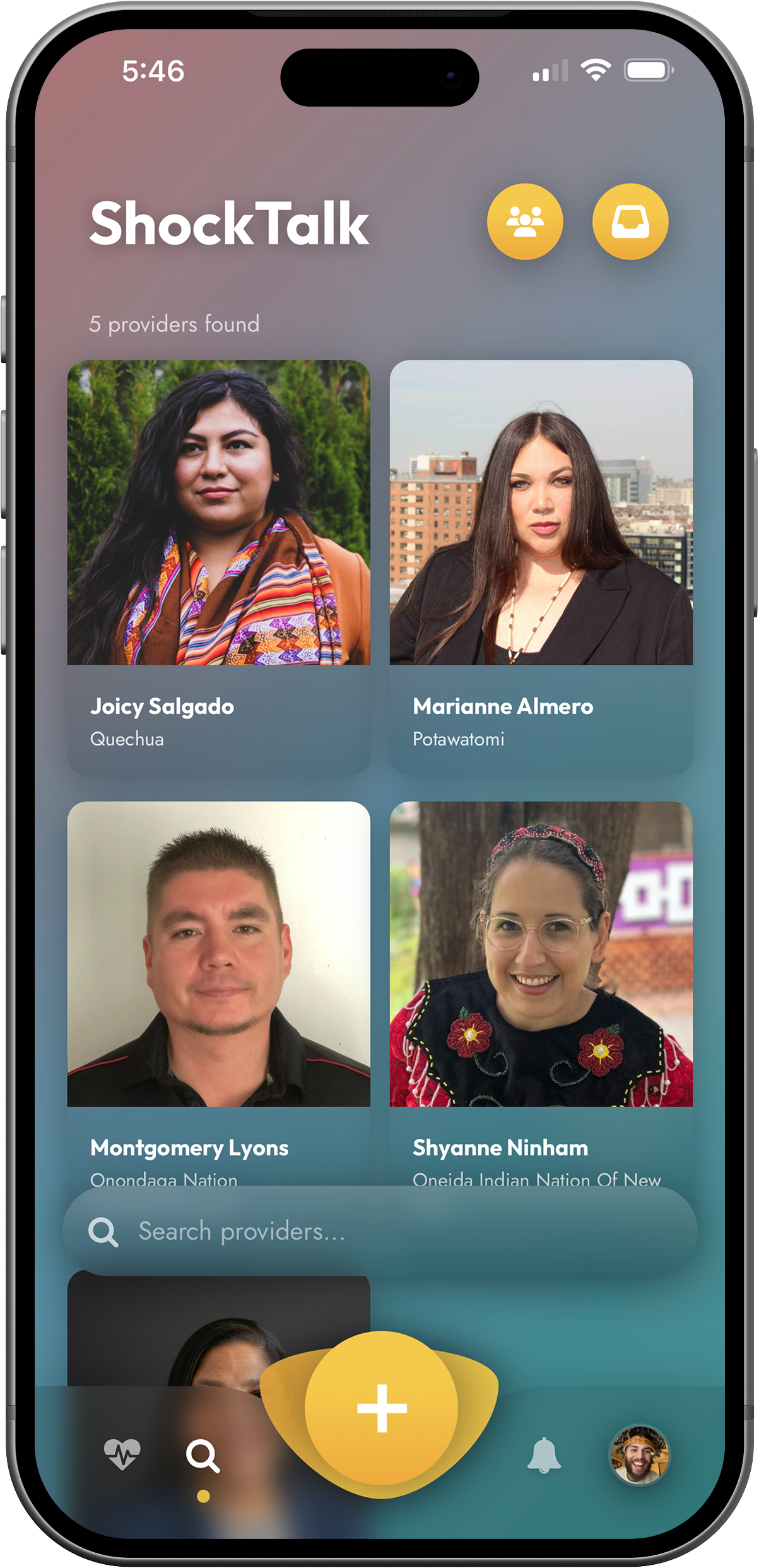
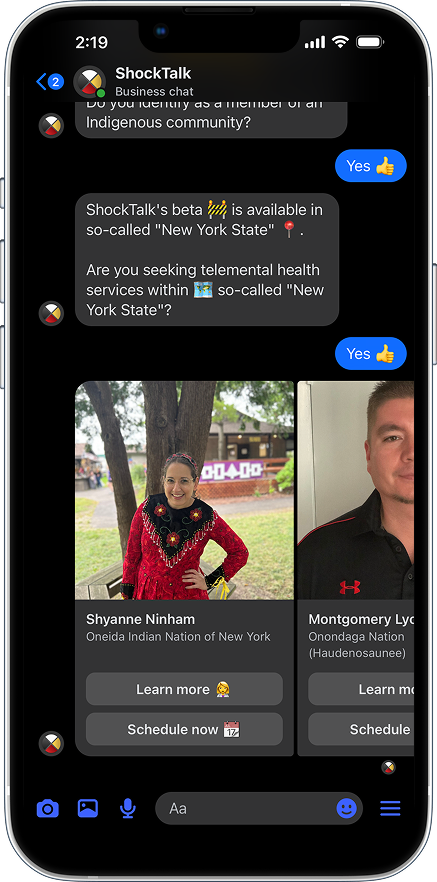
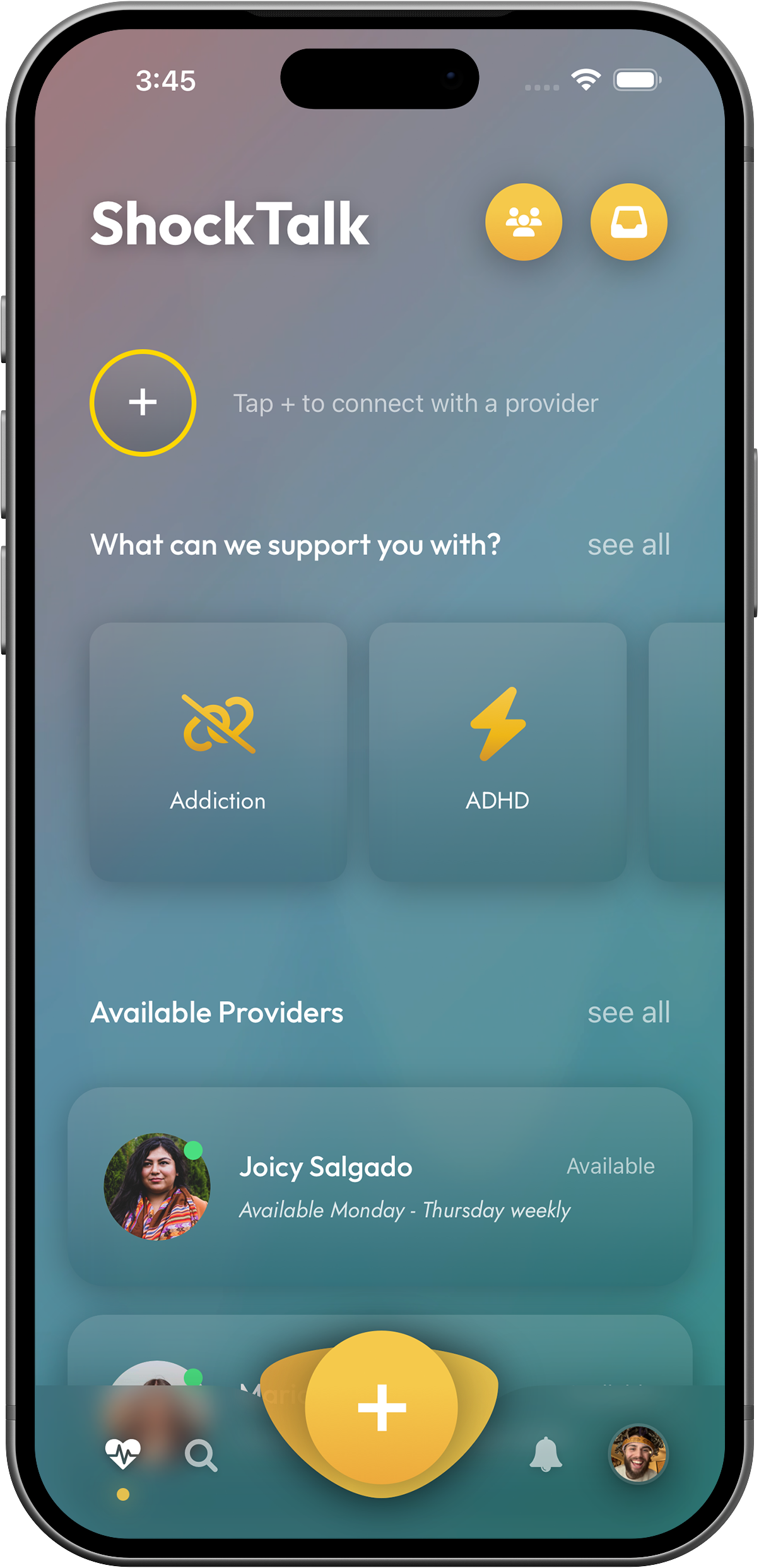
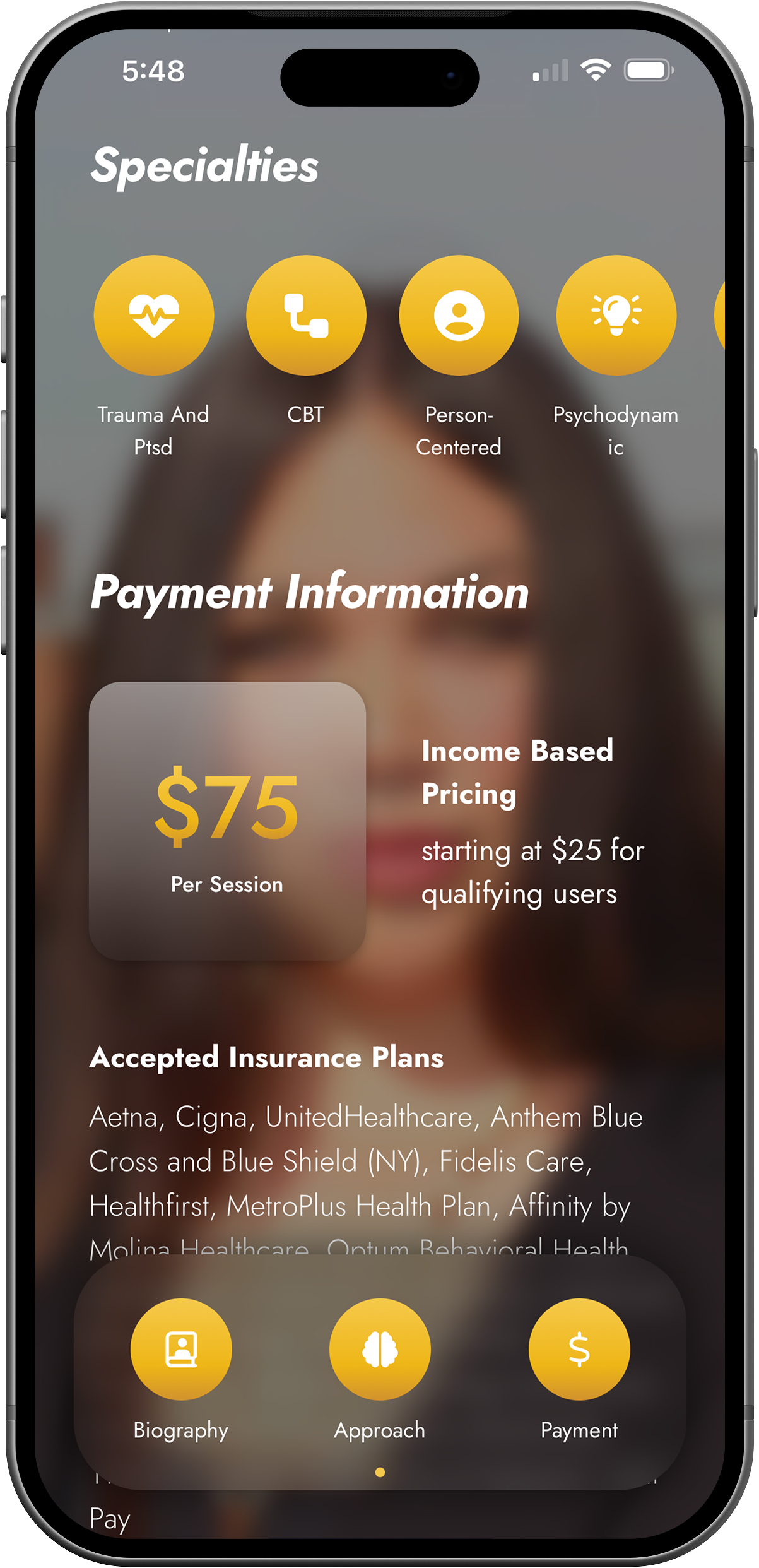
For an Indigenous person in New York City, finding mental health care often comes down to one question: how do I find an Indigenous therapist I can actually afford? Simple on the surface. But the answer fractures quickly.
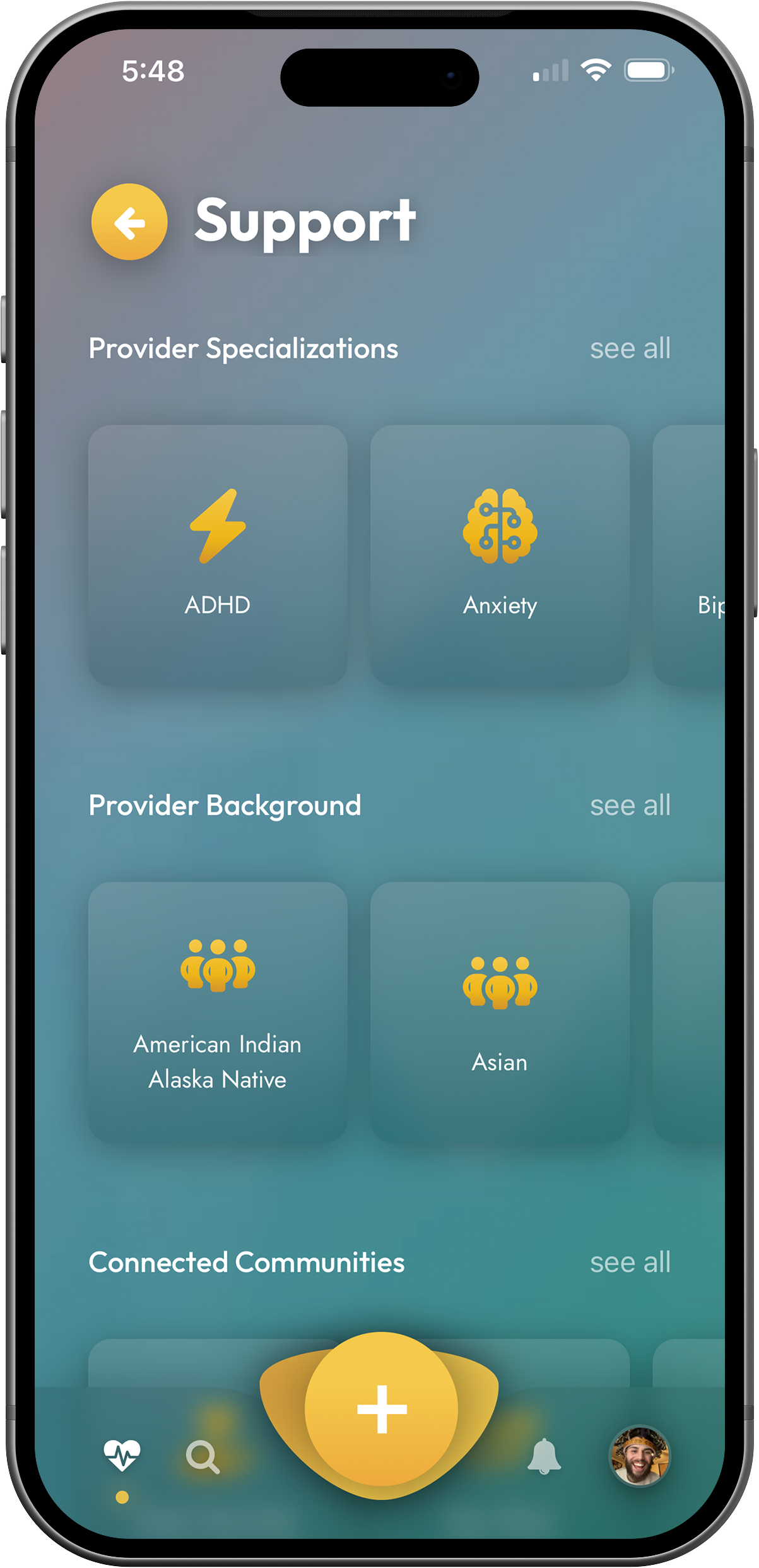
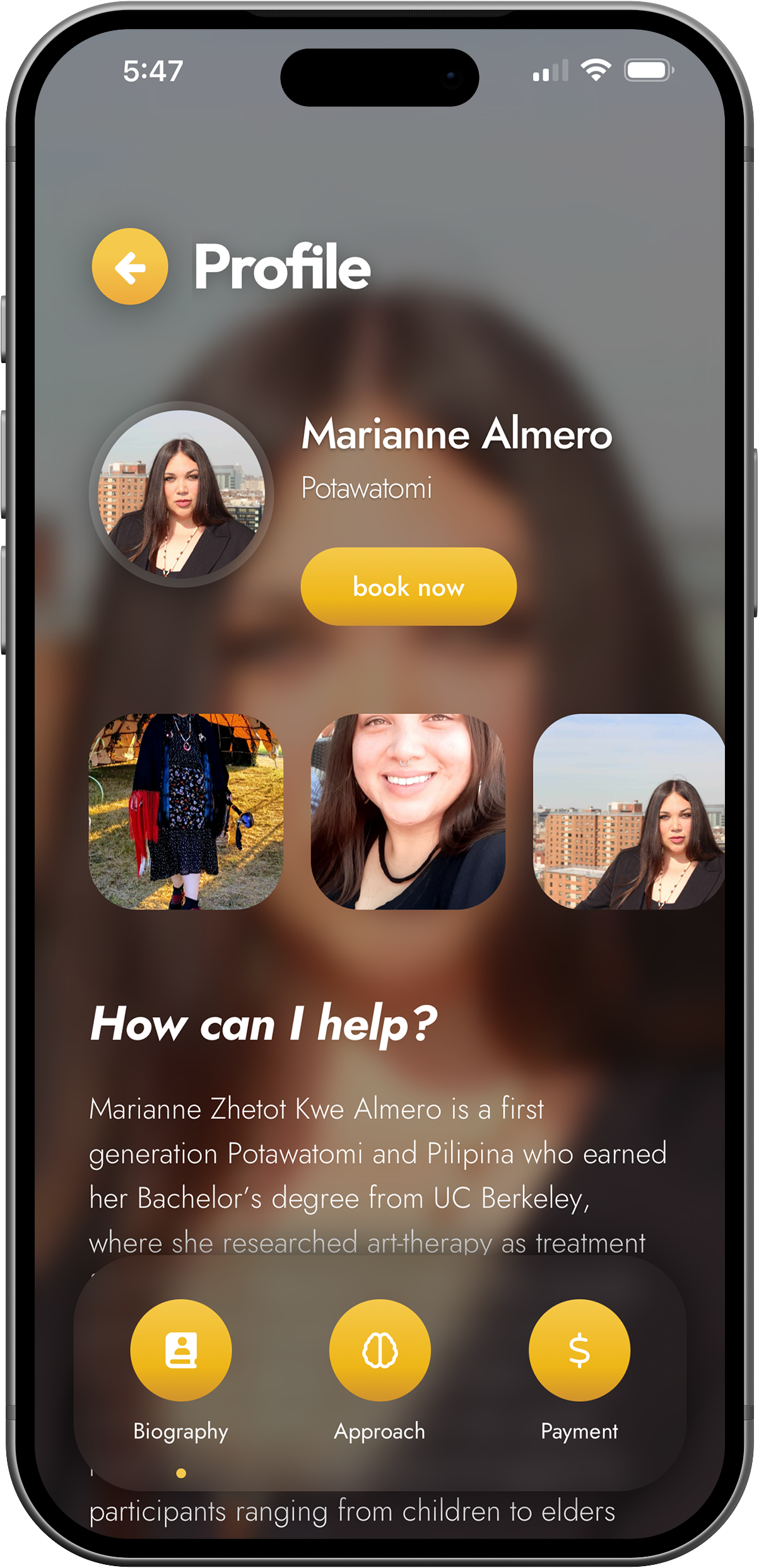
If you’re federally recognized, the nearest IHS clinic might be four hours away. If your nation isn’t federally recognized, you’re not sure where to start. If you’re Indigenous to Central America, the Caribbean, or the Pacific Islands, you’re not sure there’s anything out there for you at all. And even if you find someone — how do you know they’re connected to community the way they say they are?
No dedicated platform existed to answer any of these questions. With IHS funded at less than half its required budget and only 1–2% reaching urban programs — despite more than 70% of Indigenous people living in urban areas — there was no institutional backstop either.
The system wasn’t built for them. ShockTalk was.